























When to Choose Surgery vs Non-Surgical Treatment

An Achilles tendon rupture is a serious injury that can significantly affect walking, sport, and daily function. Choosing between surgical and non-surgical treatment depends on several factors including the type of rupture, patient activity level, and timing of diagnosis.
Achilles tendon connects the calf muscles to the heel bone and is essential for walking, running, and jumping. A rupture occurs when the tendon partially or completely tears, often during sudden acceleration or change of direction.
Common symptoms include:
- Sudden sharp pain or “pop” in the back of the ankle
- Feeling of something/someone kicked you in the back of the ankle
- Difficulty walking or pushing off the foot
- Swelling and bruising
- Weakness or inability to stand on tiptoes
Achilles tendon ruptures usually occur at two locations:
- Mid portion tendon rupture: this area is known to have a higher incidence of rupture as it has reduced blood supply compared to other areas of the tendon
- Insertional tendon rupture – this is less common but occurs when the tendon ruptures from the insertion on the calcaneus/heel bone.
Non-Surgical Treatment for Achilles Tendon Rupture
Non-surgical (conservative) management is increasingly used in selected patients and involves functional rehabilitation. If diagnosed within 48-72 hours of injury and treated appropriately, an early functional rehabilitation program may be prescribed as treatment.
When Non-Surgical Treatment May Be Appropriate
Non-surgical treatment may be recommended when:
- The rupture is partial
- The gap of the ruptured tendon ends is less than 20mm (MRI or Ultrasound)
- Location of rupture – midportion vs insertional rupture
- The injury is diagnosed early – within 48-72 hours and a raised CAM boot is applied
- The patient is less physically demanding or active
- Surgical risk is higher due to medical conditions
Non-surgical treatment will involve a specific rehabilitation program which will be a combination of non weight bearing in a boot – transitioning in a specialised boot for a period of 8-10 weeks with a structured physiotherapy program.
Non surgical treatment has some advantages when compared to surgical treatment which include reduced risks of infection, nerve injury and wound problems. Non surgery has similar long-term outcomes in selected cases and suitable for many patients when managed correctly.
Surgical Treatment for Achilles Tendon Rupture
Surgical repair of the Achilles tendon involves re-approximating the torn tendon ends to restore strength, function and length. Surgery for Achilles tendon ruptures is normally advised when:
- Chronic presentation to the surgeon (injury is weeks or months old)
- The rupture is complete and the gap between the two ends is large (the tendon stump can retract up the back of the leg in some cases )
- The patient is younger, athletic, or highly active
- Location of the rupture – insertional ruptures are more likely to need surgery then mid portion rupture.
- Faster return to sport is desired
- Non-surgical treatment has failed
Surgery Vs Non Surgery
Depending on your presentation and investigations, the surgeon will determine which treatment option that will be more suitable. Surgical repair reports a slightly lower re-rupture rate (2-8%) then non surgical treatment (10-14%) for the tendon rupture. Surgery may also allow a slightly quicker return to activity and improved long term strength. Surgical management also has the added complications of the chance of getting an infection, swelling, post-operative pain and bleeding.
Regardless both options will require a very similar recovery timeline in the specialised CAM boot before being able to return to activities and gaining full function and strength.
Case Study: Surgery vs Non Surgery (Two patients that presented to Dr Kak)
-
Case 1: 41 year old male
- Active, plays social sports 3-4x a week including basketball and tennis
- Ruptured his Achilles tendon – midportion level (Ultrasound showed tendon rupture with a 10mm gap) with an additional split tear within the distal tendon stump
- Diagnosis was made 24 hours after injury
- Placed into a 30 degree wedge VacoPed boot & non weight bearing
- Followed a strict rehabilitation program and physiotherapy
- Returned to weekend sports 7-9 months after injury
- Reason for Non Surgery: Gap was <20mm, diagnosis was made early and a wedge boot worn within 24 hours, patient is healthy and not playing elite level sport, location of rupture was midportion and not insertional
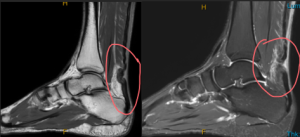
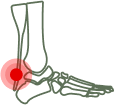
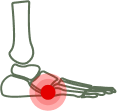
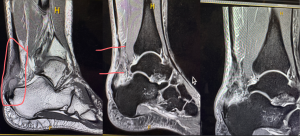
Figure1 and 2: MRI T1 and T2 weighted sagittal view showing the full thickness rupture of the tendon.

Figure 3: VacoPed boot to be worn in the rehabilitation process
-
Case 2: 49 year old male – healthy.
- Active, father of 4, plays social sports 4-5x a week squash, oztag and tennis
- Was playing Oz tag and felt a pop in the back of his ankle
- Was placed in a raised CAM boot within 24 hours but awaiting MRI results
- MRI confirmed full rupture from the insertion and a 4.5cm retraction of the proximal stump
- Surgery was advised given the location of the rupture and the substantial retraction of the tendon
- Tendon was repaired and attached back into the calcaneus (heel bone) using a bone anchor. Non WB in a cast for 2 weeks and then commenced rehabilitation program in the raised boot
- 10 weeks post op walking in regular shoes
- Reason for surgery: Rupture was at the insertion, the gap between the two stumps was large (45mm), large split tear and avulsed bone within the distal tendon stump

Achilles Tendon Rehabilitation Protocol
For a detailed rehabilitation timeline following Achilles tendon rupture treatment, view our structured rehabilitation protocol. This guide outlines the recommended recovery stages and physiotherapy progression to support safe healing and return to activity.